Significant risks and stressors exist at the point of drug preparation and administration.
Simplist® ready-to-administer (RTA) prefilled syringes simplify the process and reduce the opportunity for error.1
- Ready-to-administer
- Manufacturer-prepared
- 18–, 24–, or 36–month shelf life
- Single unit dosing
- Tamper-evident packaging
Simplist is associated with a 4x lower error rate* compared to traditional practice, including a cartridge-based systems1
4x
lower error rate
A prospective, multisite, observational study of IV push medication preparation and administration compared the error rates between ready-to-administer products and traditional practice, including a cartridge-based syringe system and vial and syringe.
- Simplist was the only RTA delivery system used in the study
- Study limitations include only a select number of sites (3) and steps observed
Ready-to-administer delivery system benefits2
Medication Safety
- Fewer steps and manipulations, minimizing contamination and limiting the opportunities for medication errors2,3
- Optimizing product presentations with single unit doses may reduce waste and financial burden4
- Adherence to safety guidelines2
- Labeled and barcoded to help verification of proper drug and dose prior to administration, promoting safe medication delivery2
RTA medication systems are recommended by leading independent medication safety associations and professional organizations.4,5,6,7
The Joint Commission
Whenever possible, have medications available in ready-to-administer form.4
CMS State Operations Manual
Whenever possible, medications shall be available for inpatient use in single-unit packages and in a ready-to-administer form. Manipulation of medications before administration by final users should be minimized.5
American Society of Health-System Pharmacists
Whenever possible, medications are dispensed in the most ready to administer form available from the manufacturer.6
Institute for Safe Medication Practices
To the greatest extent possible, provide adult IV push medications in a ready-to-administer form (to minimize the need for manipulation outside of the pharmacy sterile compounding area). Do not withdraw IV push medications from commercially available, cartridge-type syringes into another syringe for administration.7
MicroVault® packaging supports secure dispensing of controlled substances
Simplist prefilled syringes in MicroVault tamper-evident packaging provides options that may help enable product size optimization in a consistent drug delivery system across our portfolio.
Omnicell® Controlled Substance Dispenser (CSD) accommodates Simplist MicroVault prefilled syringes
The Controlled Substance Dispenser provides additional levels of security for single dose dispensing of high-risk, high-value medications.
Learn more
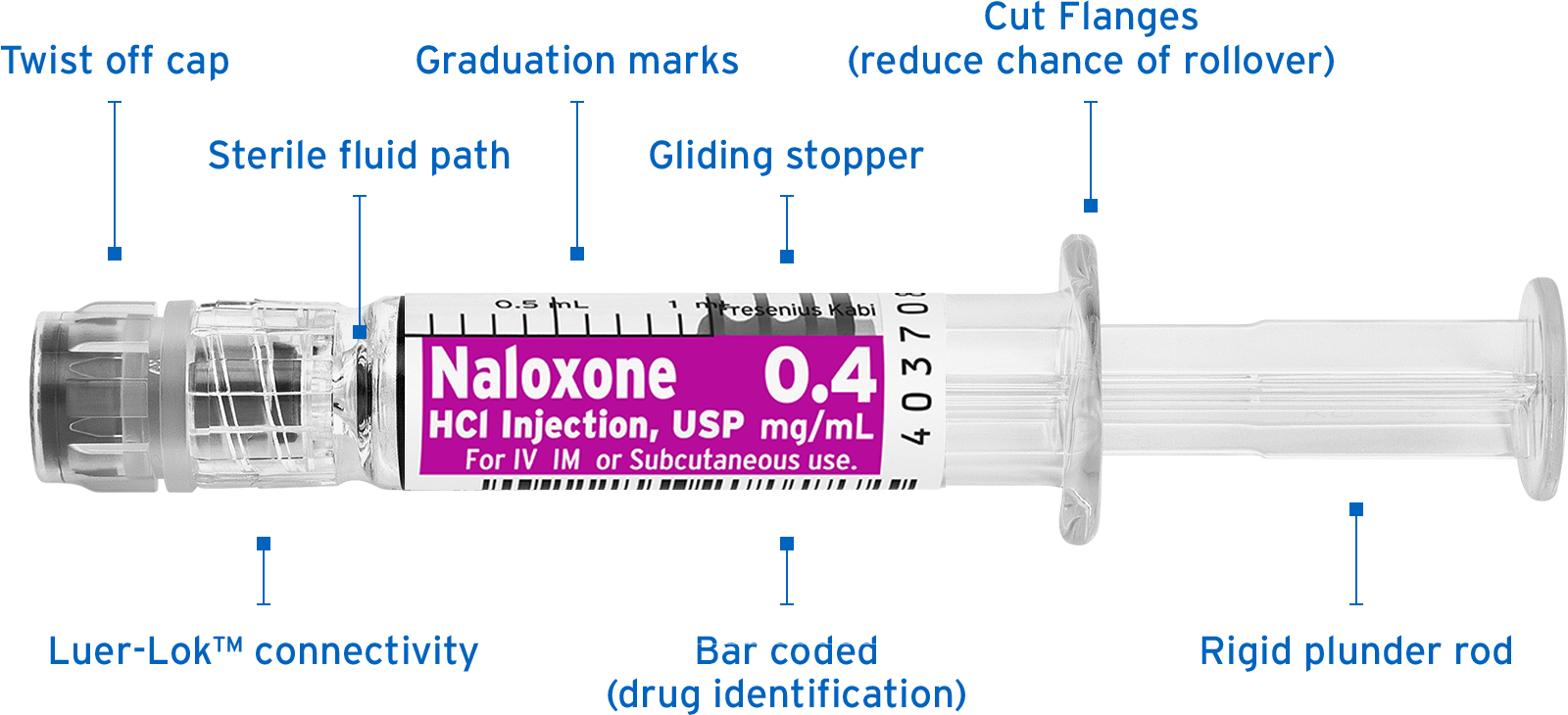
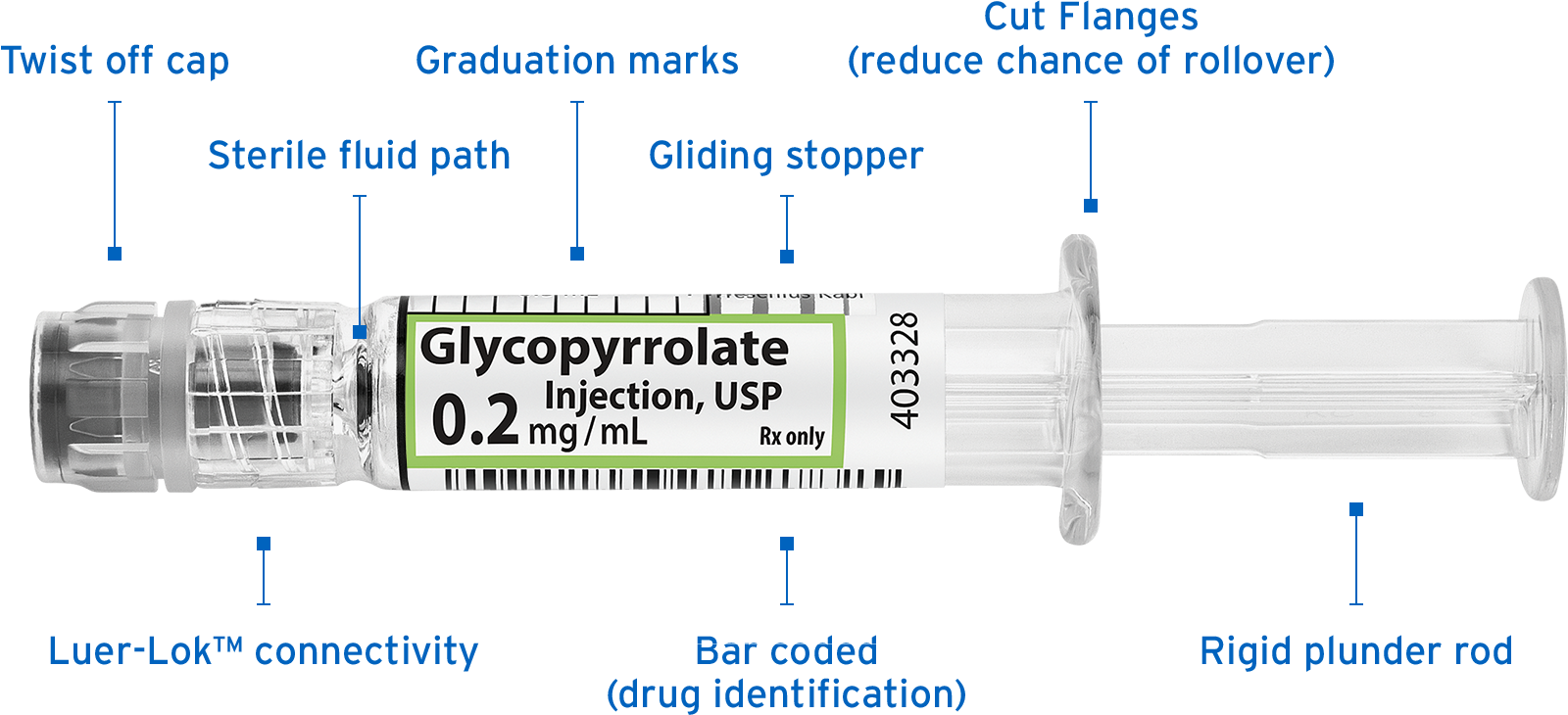
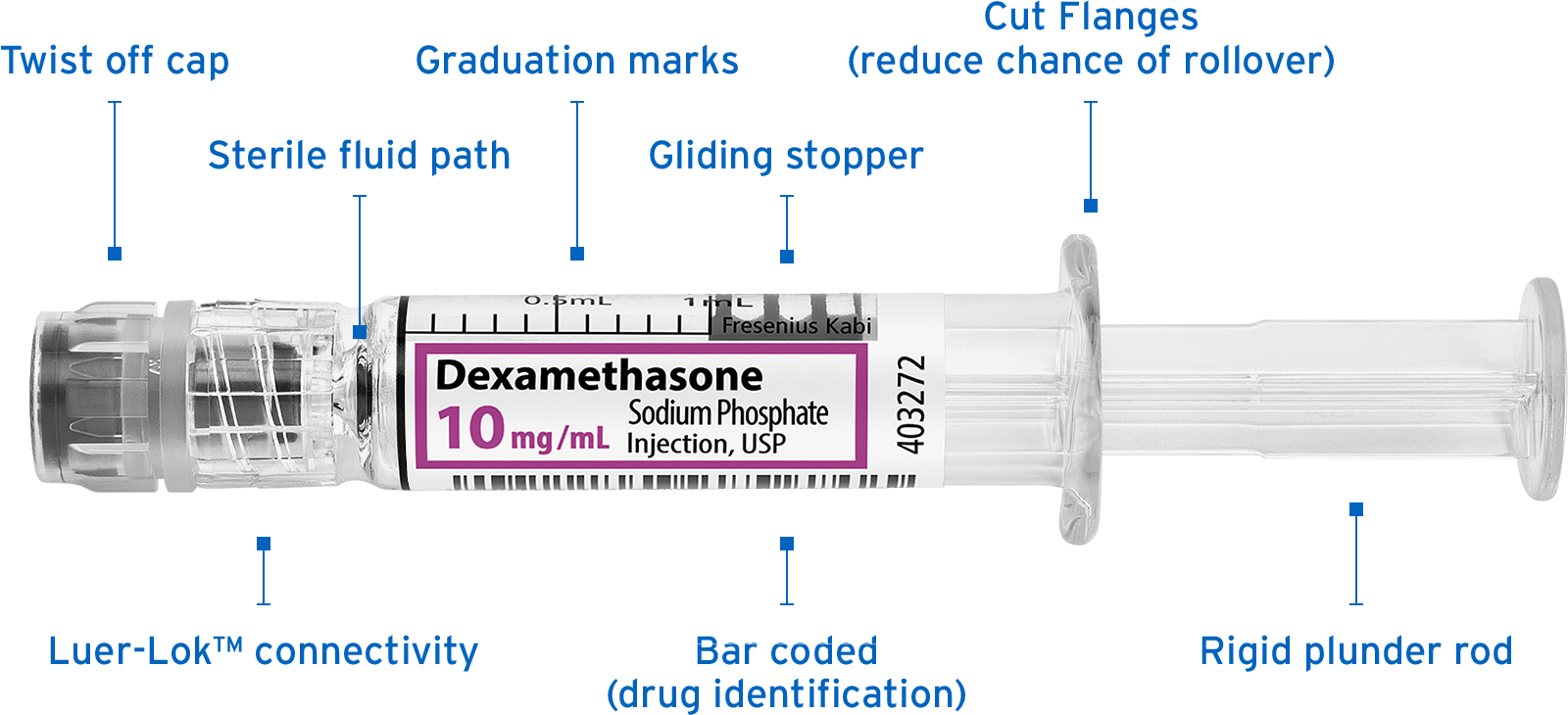
Blister packaging with clear, easy-to-read labels may help ensure delivery of the right medication at the right dose
Each Simplist prefilled syringe and blister are color coded and identically prelabeled with the drug name, strength, expiration date, and barcode to assist with drug identification.
 Explore products
Explore products

Simplist MicroVault Instructions for Use Training Video
Watch the video